By Mike Davies
The covid-19 pandemic is not a surprise. There are hundreds of strains of coronavirus, most of which only affect animals. Ever since the outbreak of Sars in 2002, and of Mers (or camel flu) a decade later, scientists have been warning that climate change, urbanisation, and international air travel create the perfect breeding ground for infectious and cross-diseases.
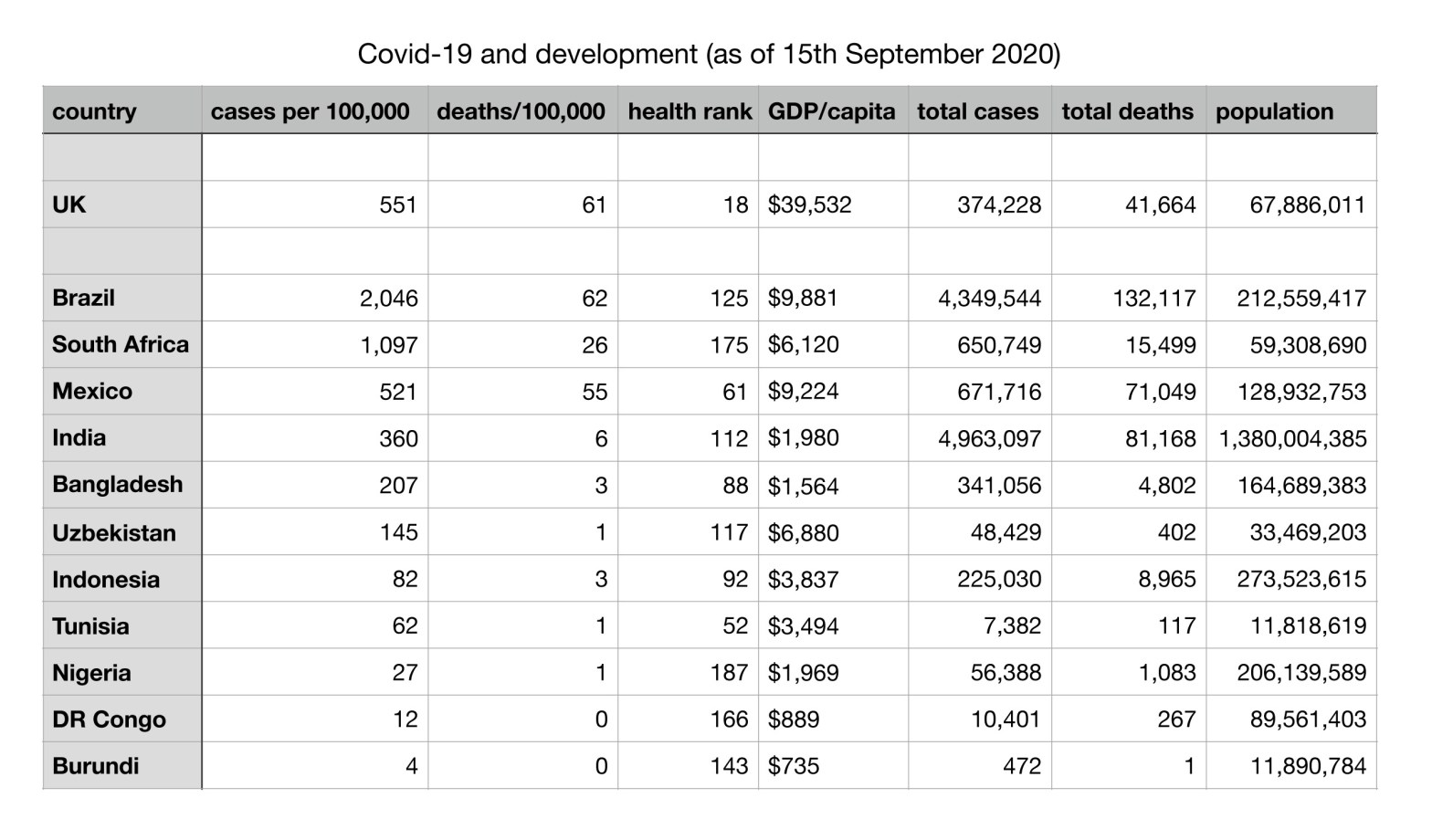
It is surprising, however, that many poorer countries in the developing world have managed to contain the spread of infection more successfully than the United States, the United Kingdom and other rich western countries. The table above shows covid-19 cases per 100,000 of population and deaths attributed to covid-19 per 100,000 of population, as at 15th September 2020, across a sample of countries with per capita Gross Domestic Product (GDP) less than a quarter of that of the United Kingdom – plus the UK for comparison. Note that the ‘headline figures’ for cases and deaths are per 100,000 of population to make comparisons fair across countries.
Of course, there are certain reservations that go with any such set of figures. Reporting approaches vary across countries. So does the capability to compile accurate reports, including the ability to diagnose. There are differing political and other pressures: perfect reporting can hardly be expected in war-torn Congo.
Nonetheless, you might reasonably expect poorer countries (with lower GDP per capita) to have worse covid figures than richer countries. Poorer countries tend to have less good hygiene facilities, lower levels of education, a stronger economic incentive to carry on regardless, plus a weaker health-care system more easily overwhelmed. (The ‘health rank’ column in the table is taken from a World Health Organisation report on national health systems.)
In fact, the opposite seems to prevail. In general, the lower a country’s GDP per capita (i.e. the poorer it is) the lower its rate of covid infections and the lower its death rate from covid. There even seems to be little correlation between the ranking given to a country’s health care system and its rates of infection and death from covid. You might expect countries with a better ranking to have lower rates of infection and death, but the figures do not appear to support this expectation.
The surprising figures may simply be a matter of geography and communications. The initial spread from China’s Wuhan province largely followed land and air routes, including entering Europe in force via an Italian ski resort. Early infections became a centre from which the infection spread. In that hypothesis, the most significantly infected country in Africa – the Republic of South Africa – simply had better air connections than the rest of the continent. Of course, the September figures tell nothing like the whole story. It may be that countries currently with few cases and few deaths are not ‘lucky’ but merely ‘late’.
Alternative hypotheses include weather. Many less developed countries have climates significantly different from, say, Britain. However, the relentless increase of infection in the United States, which embraces a wide range of climates, including the very hot, suggests this is unlikely.
Another possibility is genetic. Certainly there are significant variations among populations in susceptibility to some diseases, such as sickle cell anaemia and malaria. The UK infection rate suggests higher levels of susceptibility among black and ethnic minority populations. But this hardly explains low infection rates in, say, African countries.
There are decisions now being made in developed countries that will heavily impact less developed countries. The politics and economics of those decisions matter to us all.
Firstly, availability of vaccines at affordable prices. If rich countries buy up stocks of vaccines when they become available, there may be none for developing countries. Even if stocks are available, their pricing will be crucial. If big pharma sets prices on a capitalist model, developing countries will be unable to afford them in the necessary quantities.
Secondly, drugs to treat covid are emerging. By chance, one of the earliest, dexamethasone, is already available and fairly cheap. But how will other treatments be priced and will they even be available outside the developed world?
Some players in this game are openly nationalistic, with the ‘devil take the hindmost’ attitude of Donald Trump, though he claims to have had a kind of conversion (‘I get it – and I understand it’) on the way to hospital earlier this month. Others make more encouraging noises. But even the encouraging ones, like Britain, are busy buying up vaccine and treatment stocks and pre-ordering more, to supply their own citizens before others.
Politically any approach that sets out to corner stocks is unacceptable. It would condemn people to death simply because they live in a poor country. Even for those willing to ignore the ethics, withholding vaccine or treatment from the developing world is not a good idea. Creating reservoirs of potential or actual infection in the developing world leaves rich countries vulnerable to a resurgence. Covid carries no passport.
Even for a rich country like Britain or the US, the economic effects of covid are huge and will remain so for a long time. Already the British government has committed £200 billion, millions are out of work, and companies are cutting back or closing down.
For any developing country hit by covid, the impact is likely to be even more severe, with the government less able to intervene to mitigate the damage. Further, just as the impact of the Great Depression had grave knock-on effects across the globe, the consequences of covid will ripple out disastrously to less developed countries.
How much priority will the UK, US and European Union give to mitigating the effects of covid on the poorer countries of the world?
Covid should not be seen simply as an event that kills large numbers of people. Rather, it should be seen as something that exposes the frailties of humanity’s whole approach to life.
This pandemic is not some sort of unpredictable one-off, outside the scope of things we should prepare for. Such events are clearly going to recur. In just the last two decades we have seen Severe Acute Respiratory Syndrome (Sars, 2002), Middle East Respiratory Syndrome (Mers, 2012), and the current Severe Acute Respiratory Syndrome Coronavirus 2 (covid-19). These have all been associated with close contact between humans and wild animals. Cross-over diseases are rare, but still happen dangerously often. Remember that some of our ‘traditional’ diseases, such as cowpox/smallpox, came from close contact with domesticated animals.
Such close contact is a growing reality as humans cut ever more deeply into the living space of wild animals and as our grossly unequal society encourages increasing use of wild animals for food. Our bodies are not prepared for a disease they have never encountered before. All it needs is the right combination of high enough infectivity and a mortality rate not so high as to wipe out its hosts too quickly (but still high enough to threaten millions). Sars and Mers were either not infectious enough or too lethal. Covid-19 fitted the bill nicely.
There will, of course, be ‘technical’ ways to address covid: vaccines and treatments. We might even get to retain some of our civil liberties, if we are lucky. But the way for humanity to avoid a succession of lethal pandemics does not lie primarily in research labs, hospitals and street wardens.
Humanity needs to regain its respect for the natural world and cease to believe that because we are intelligent we have an unconstrained right to smash up our planet and its other species. We must forget about ‘domination over them’ and learn to respect them and give them space.
Mike Davies is the Chair of the AGS
